
Introduction
You’ve tried countless hair loss treatments—minoxidil, supplements, expensive shampoos—yet your hair continues to thin. You’re not alone in this frustration. The real reason nothing you’ve tried has stopped your hair loss likely stems from overlooked factors that most solutions ignore. Whether it’s misidentifying your specific type of thinning, using incomplete treatment approaches, or missing critical hormonal influences, standard remedies often fail without proper medical guidance. This article reveals what hair specialist Doctors know about effective treatment strategies, from understanding different hair loss patterns to creating personalised solutions that actually deliver results you can see.
Key Takeaways – TL/DR
- Most hair loss treatments fail because they target symptoms, not the underlying type of hair loss
- 85% of people misidentify their hair loss type, leading to ineffective treatment choices
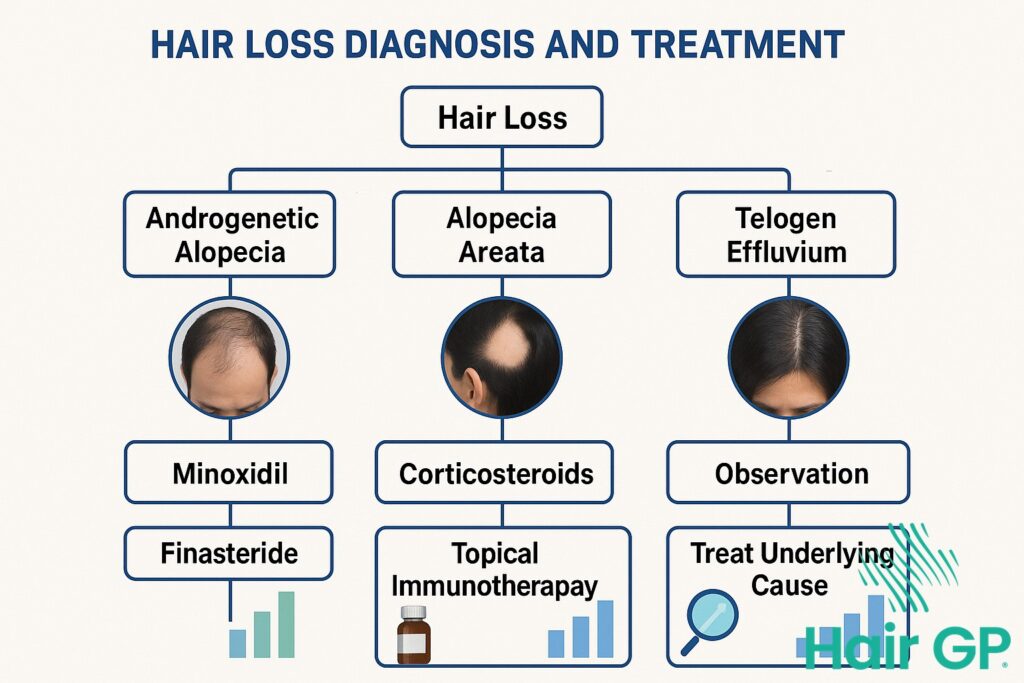
- Androgenetic alopecia requires DHT blockers like finasteride, while telogen effluvium needs different approaches
- Combination therapy addressing multiple pathways shows 3x better results than single treatments
The Real Reason Nothing You’ve Tried Has Stopped Your Hair Loss
The truth about unsuccessful hair loss treatments lies in their generic approach to a deeply individual problem. Most over-the-counter solutions target DHT and testosterone broadly, ignoring that up to 70% of cases involve multiple contributing factors beyond simple genetics [1].
Why One-Size-Fits-All Solutions Don’t Work
The real reason nothing you’ve tried has stopped your hair loss stems from fundamental biological variations between individuals. Your genetic makeup determines how hair follicles respond to DHT, with certain gene variants affecting treatment response rates by up to 40% [2]. Additionally, testosterone metabolism varies significantly based on enzyme activity levels unique to each person.
Without proper hair loss diagnosis, treatments miss critical factors. Your specific pattern among various types of hair loss requires targeted intervention. Lifestyle factors—stress, nutrition, sleep quality—modify how treatments work at the follicular level. This explains why identical treatments produce vastly different results across individuals, making personalised assessment essential for breaking the cycle of treatment failure.

Understanding Your Type of Hair Loss
Correctly identifying your specific type of hair loss determines whether treatment will succeed or fail. Most people unknowingly treat the wrong condition, particularly when androgenetic alopecia mimics telogen effluvium or vice versa, leading to months of ineffective remedies.
Signs You’re Treating the Wrong Type
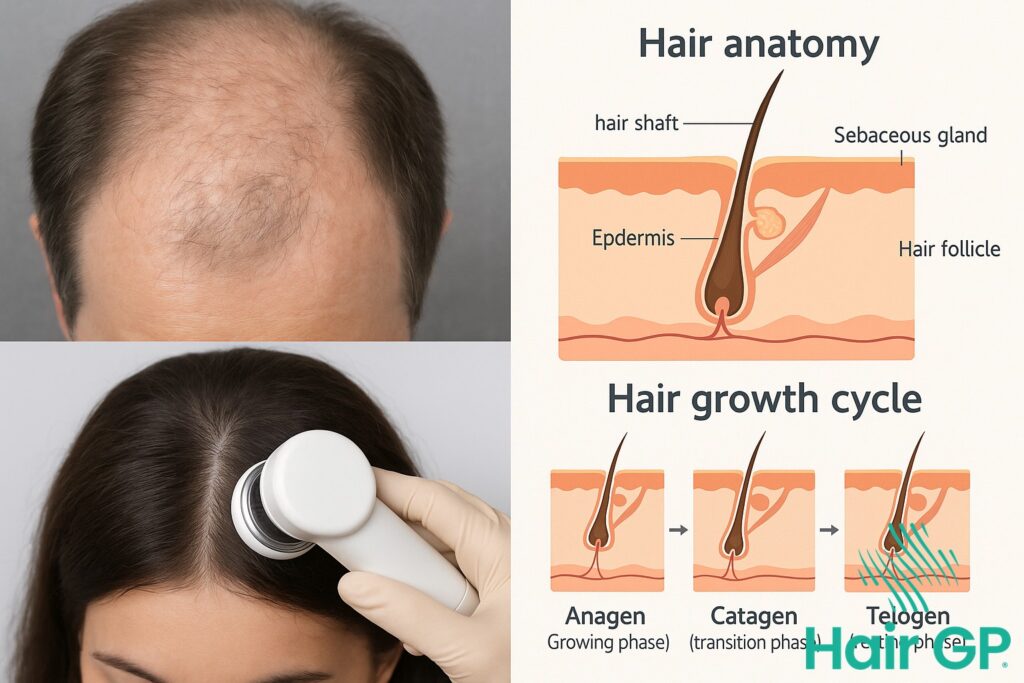
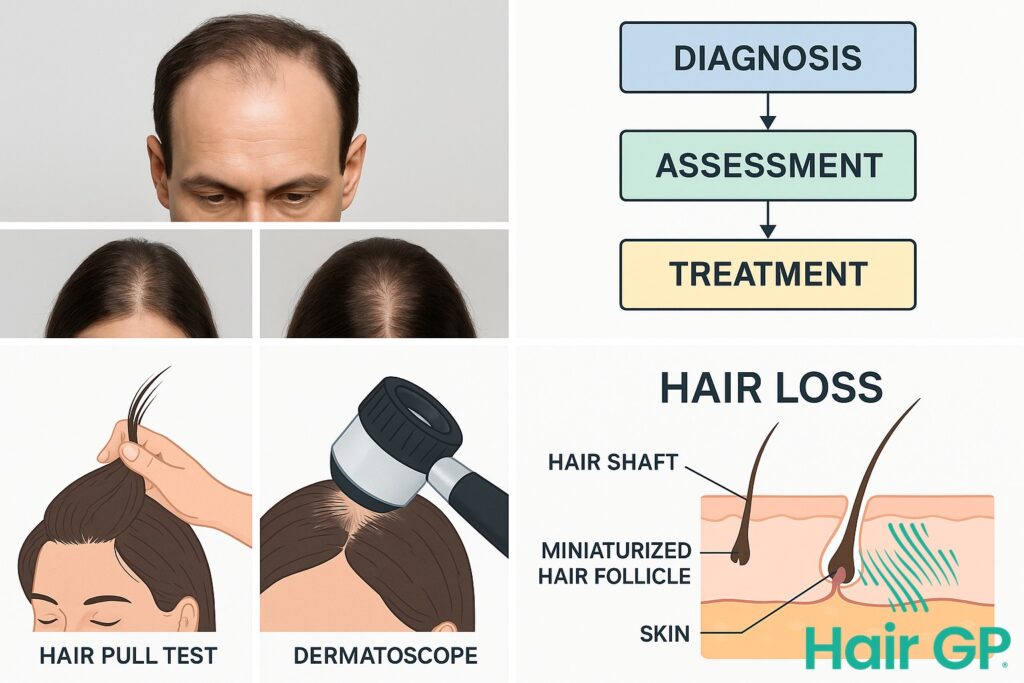
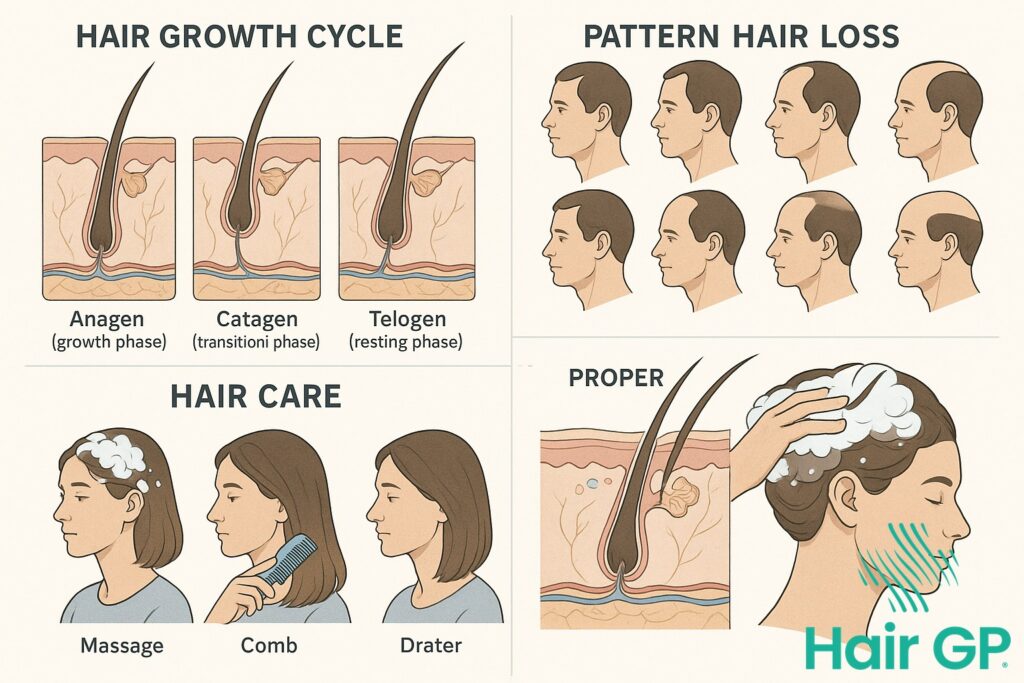
Several indicators reveal when your current approach doesn’t match what’s actually causing your thinning. Androgenetic alopecia follows predictable patterns—crown thinning in male pattern baldness or diffuse central thinning in women—whilst telogen effluvium creates sudden, widespread shedding [3]. The timing matters: genetic loss progresses gradually over years, reducing follicles’ diameter progressively, whereas stress-triggered telogen effluvium happens within three months of a triggering event [4]. If minoxidil hasn’t improved your condition after six months, you’re likely addressing the wrong type. Response patterns provide crucial clues—androgenetic alopecia partially responds to DHT blockers whilst telogen effluvium resolves once the underlying trigger is addressed. Misidentification wastes precious time whilst follicles continue deteriorating.

Female Pattern Hair Loss: Why Standard Treatments Often Fail
Female pattern hair loss presents unique treatment challenges that standard approaches frequently overlook. Unlike male-pattern baldness, women experience complex hormonal shifts throughout life—from menstruation to pregnancy, post-partum, and menopause—each affecting hair growth differently [1]. These fluctuations make single-target treatments ineffective, as the underlying hormone balance constantly changes. Standard minoxidil formulations, whilst helpful, often fail to address the oestrogen-androgen interplay crucial to women’s hair health.
Medication limitations further complicate treatment. Finasteride, highly effective in men, remains contraindicated for pre-menopausal women due to pregnancy risks [5]. Post-partum telogen effluvium, affecting up to 50% of new mothers, requires entirely different management than chronic female pattern hair loss. Many women unknowingly combine incompatible treatments or miss critical windows for intervention. Comprehensive hormone testing reveals individual patterns that generic treatments cannot address, explaining why what works for one woman may fail for another despite similar symptoms.

Hair Loss Treatments: Why Minoxidil and Finasteride Aren’t Enough
Whilst minoxidil and finasteride remain the gold standard hair loss treatments, relying on either medication alone often delivers disappointing results. Clinical studies show monotherapy achieves satisfactory outcomes in only 30-40% of patients [6], highlighting why comprehensive treatment strategies consistently outperform single-agent approaches.
Building an Effective Treatment Plan
Success requires systematically combining proven interventions based on your specific hair loss pattern. Start by establishing baseline measurements through standardised photography and density assessments. Track monthly progress indicators including shed reduction, miniaturisation reversal, and coverage improvement. Most patients see initial results within three to four months, though optimal outcomes typically require 12-18 months of consistent treatment [7].
Adjust dosing and add complementary therapies based on response patterns. Consider microneedling to enhance minoxidil absorption, low-level laser therapy for follicle stimulation, or specialised shampoos targeting scalp inflammation. This multi-modal approach addresses different pathways simultaneously, significantly improving success rates compared to finasteride or minoxidil alone.
Telogen Effluvium: The Overlooked Temporary Hair Loss
Telogen effluvium causes temporary shedding when physical stress—surgery, illness, childbirth—or emotional trauma disrupts follicle cycling. Unlike pattern baldness, DHT blockers provide no benefit since androgens aren’t involved [8]. Most experience recovery within 3-6 months following stress resolution [9]. Recognising this distinction prevents unnecessary treatment while managing underlying stress-hair-loss triggers. The natural recovery timeline requires patience as follicles gradually return to normal growth phases.
Taking Action: Your Personalized Hair Loss Solution
Taking action against hair loss starts with booking an appointment to talk with your GP or specialist doctor. Come ready with photos documenting changes over the past six months and a detailed log of symptoms, medications, and family history. This preparation ensures productive discussions about evidence-based treatments suited to your specific condition.
Your doctor can order appropriate blood tests, perform scalp examinations, and create a personalised treatment plan with realistic timelines. Start tracking progress monthly using standardised photos and measurements—most effective treatments require three to six months for visible results. Remember, successful treatment relies on accurate diagnosis followed by consistent application of proven therapies, not quick fixes or unverified remedies.
Conclusion
Evidence-based hair loss treatment requires professional diagnosis for optimal benefit. Don’t guess—seek expert support to identify your specific condition. With proper evaluation and targeted approaches, effective solutions exist. Schedule your professional consultation today to begin your personalised treatment journey.
Frequently Asked Questions
Most proven treatments require 3-6 months for visible improvement, with optimal results at 12 months
Stress typically causes temporary telogen effluvium, but chronic stress can worsen genetic hair loss
References
- Gupta AK, Talukder M, Venkataraman M, Bamimore MA. Minoxidil: a comprehensive review. J Dermatolog Treat. 2022;33(4):1896-1906.
- Heilmann-Heimbach S, Hochfeld LM, Paus R, Nöthen MM. Hunting the genes in male-pattern alopecia: how important are they, how close are we and what will they tell us? Exp Dermatol. 2016;25(4):251-257.
- Asghar F, Shamim N, Farooque U, Sheikh H, Aqeel R. Telogen Effluvium: A Review of the Literature. Cureus. 2020;12(5):e8320.
- Malkud S. Telogen Effluvium: A Review. J Clin Diagn Res. 2015;9(9):WE01-3.
- Kanti V, Messenger A, Dobos G, et al. Evidence-based (S3) guideline for the treatment of androgenetic alopecia in women and in men – short version. J Eur Acad Dermatol Venereol. 2018;32(1):11-22.
- Gupta AK, Mays RR, Dotzert MS, et al. Efficacy of non-surgical treatments for androgenetic alopecia: a systematic review and network meta-analysis. J Eur Acad Dermatol Venereol. 2018;32(12):2112-2125.
- Kanti V, Messenger A, Dobos G, et al. Evidence-based (S3) guideline for the treatment of androgenetic alopecia in women and in men – short version. J Eur Acad Dermatol Venereol. 2018;32(1):11-22.
- Asghar F, Shamim N, Farooque U, et al. Telogen Effluvium: A Review of the Literature. Cureus. 2020;12(5):e8320.
- Rebora A. Telogen Effluvium: A Comprehensive Review. Clin Cosmet Investig Dermatol. 2019;12:583-590.

")
