
Introduction
Studies reveal that up to 60% of hair loss treatments fail to produce expected results, primarily because patients begin treatment without understanding why hair loss treatments fail without correct diagnosis. Each year, millions spend thousands on ineffective remedies whilst their hair follicles continue deteriorating from unidentified underlying causes.
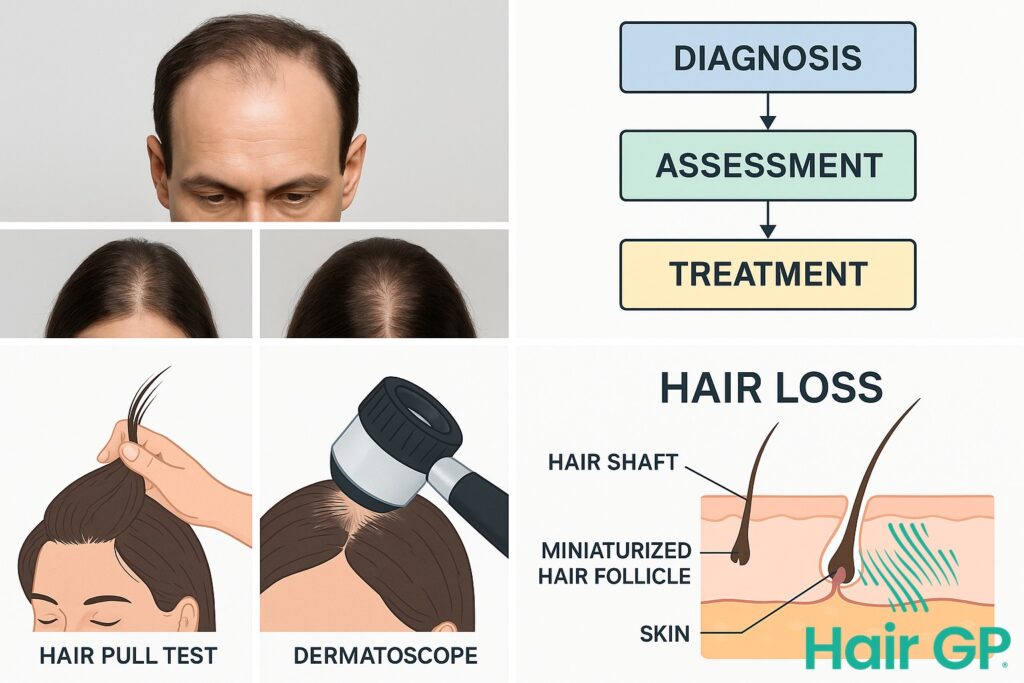
The difference between successful hair restoration and continued hair loss often lies in one crucial step: obtaining an accurate diagnosis before starting any treatment. Different types of hair loss require fundamentally different approaches—what works for genetic pattern baldness may worsen autoimmune conditions, and treatments for stress-related shedding won’t address nutritional deficiencies affecting follicle health.
This comprehensive guide explores how proper diagnostic procedures distinguish between various hair loss causes, from androgenetic alopecia to autoimmune conditions like alopecia areata. We’ll examine essential blood tests that uncover hidden medical conditions, professional examination techniques including trichoscopy and pull tests, and how dermatologists systematically identify each type of hair loss. You’ll also discover emerging treatments from clinical trials, understand which diagnostic markers determine treatment eligibility, and learn how proper hair care practices support effective treatment once the correct diagnosis is established.
Key Takeaways – TL/DR
- 70% of hair loss treatments fail when started without proper diagnosis from a Specialist Hair Doctor
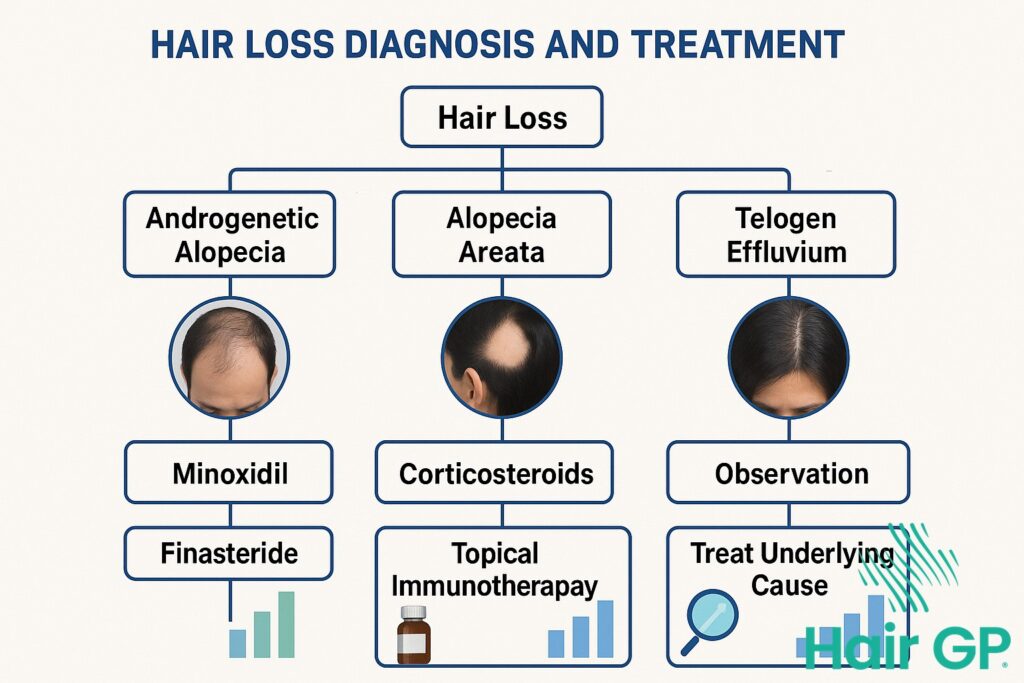
- Different types of hair loss like androgenetic alopecia and alopecia areata require completely different treatment approaches
- Blood tests and scalp biopsy can identify underlying causes that topical treatments alone cannot address
- Early accurate diagnosis can prevent permanent hair loss and scarring alopecia in many cases
Why Hair Loss Treatments Fail Without Correct Diagnosis
Without proper diagnosis, hair loss treatments become costly experiments with predictable failures. The fundamental issue lies in treating symptoms rather than causes—using generic solutions for conditions requiring specific interventions whilst underlying pathology continues unchecked.
The Hidden Costs of Trial-and-Error Treatments
The financial burden of undiagnosed hair loss extends beyond initial treatment costs. Research indicates patients spend an average of £2,400 annually on ineffective treatments before seeking professional diagnosis[1], with many cycling through over-the-counter remedies that cannot address their specific condition. When the first sign of hair loss appears, most individuals turn to generic solutions from medical literature or online forums, unaware that their genetic predisposition or underlying autoimmune condition requires targeted intervention.
Time becomes the most devastating loss. Conditions left untreated for six months show significantly reduced response rates to eventual effective treatment[2]. Androgenetic alopecia, the medical term for pattern baldness, progresses relentlessly without proper intervention, with follicular miniaturisation becoming irreversible after prolonged periods. What begins as treatable thinning evolves into permanent hair loss whilst patients experiment with inappropriate remedies.
The psychological impact compounds exponentially with each failed attempt. Studies demonstrate that repeated treatment failures correlate with increased anxiety and depression scores, creating a cycle where emotional distress potentially exacerbates hair loss conditions. Patients report feeling betrayed by their bodies and overwhelmed by conflicting information about treatment options. Professional assessment helps determine not only the correct diagnosis but also realistic expectations, preventing the emotional devastation of pursuing impossible outcomes. Understanding why hair loss treatments fail without correct diagnosis transforms the approach from hopeful experimentation to strategic intervention.

Common Causes of Hair Loss Often Misdiagnosed
Hair loss affects approximately 50% of individuals by age 50, yet studies indicate that up to 40% of cases receive incorrect initial diagnoses due to overlapping symptoms amongst various conditions. The complexity of hair loss aetiology means that conditions ranging from thyroid disease to nutrient deficiency can present identically to genetic pattern baldness, leading to ineffective treatments when the underlying cause of hair loss remains unidentified.
Nutritional Deficiencies That Mimic Pattern Baldness
Iron deficiency represents the most commonly overlooked cause, affecting up to 30% of women experiencing hair loss [3]. Serum ferritin levels below 70 ng/mL can trigger telogen effluvium despite normal haemoglobin levels, requiring comprehensive iron panels beyond basic blood tests. Vitamin D deficiency, present in 85% of alopecia patients, disrupts follicular cycling and requires levels above 30 ng/mL for optimal hair growth [4].
Protein malnutrition triggers hair shaft abnormalities within 2-3 months, whilst zinc deficiency causes diffuse alopecia that resolves with supplementation of 15-30mg daily. B-complex vitamins, particularly biotin and folate, support keratin synthesis, though isolated biotin supplementation can interfere with thyroid function tests. Hormonal imbalance from thyroid disorders affects 10% of hair loss patients, with both hyperthyroidism and hypothyroidism causing reversible alopecia. Autoimmune diseases like alopecia areata require immunological assessment, whilst chronic stress depletes essential minerals through elevated cortisol, creating a cascade of deficiency-related hair loss requiring multi-factorial treatment approaches.
Androgenetic Alopecia: The Most Misunderstood Hair Loss
Androgenetic alopecia affects 80% of men and 50% of women by age 70, yet remains widely misunderstood despite being the most common form of hereditary hair loss. This genetic predisposition to DHT sensitivity causes progressive miniaturisation that requires precise diagnosis to treat effectively, as generic approaches frequently fail without understanding individual hormonal patterns.
Female Pattern Hair Loss vs Male Pattern: Critical Differences
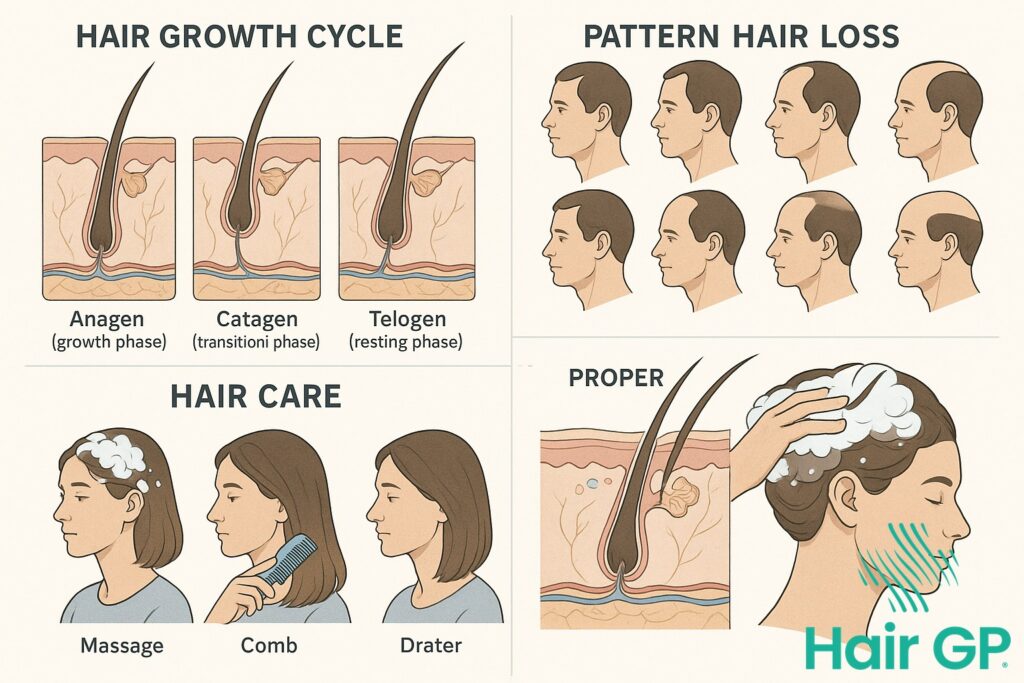
While male pattern baldness follows predictable recession patterns, female pattern hair loss presents unique diagnostic challenges requiring specialised approaches. Women experience diffuse hair thinning across the crown whilst maintaining their frontal hairline, making early detection more complex than typical male presentations[5]. Hormonal considerations differ significantly—testosterone conversion to DHT affects women differently, particularly during menopause when protective oestrogen levels decline.
Treatment limitations in women restrict options considerably. Finasteride and oral dutasteride, highly effective for male and female pattern loss in men with 85% response rates[6], require careful consideration in premenopausal women due to pregnancy risks. Minoxidil (Rogaine) remains the primary FDA-approved treatment for women, though response varies between 30-40% without proper diagnostic workup. These gender-specific differences underscore why androgenetic alopecia diagnosis must consider hormonal profiles, genetic testing, and individual presentation patterns before initiating any treatment protocol.

How Is Alopecia Areata Diagnosed and Treated
Alopecia areata presents a diagnostic challenge often confused with other hair loss conditions, despite its distinct autoimmune pathology attacking healthy follicles. This autoimmune condition occurs when the immune system mistakenly targets hair follicles, creating characteristic patches of baldness that standard hair loss treatments cannot address.
Recognising Exclamation Mark Hairs and Other Signs
Specialist Hair Doctors identify alopecia areata through specific diagnostic markers absent in other conditions. Exclamation mark hairs, broken hairs tapering towards the scalp, appear at patch borders in 44% of active cases[7]. These diagnostic features distinguish the condition from pattern baldness or telogen effluvium. Yellow dots representing keratinous debris within follicular openings provide another crucial indicator, whilst black dots indicate broken hair shafts. The pull test reveals easily extracted hairs at patch edges during active phases.
Treatment requires immunosuppressive approaches rather than conventional remedies. Corticosteroid injections directly into the bald spot achieve regrowth in 60-67% of limited patchy hair loss cases[8]. However, the unpredictable nature means patches may resolve spontaneously or progress despite intervention. Systemic immunotherapy options exist for extensive involvement, though response varies considerably. Support resources prove essential given the emotional impact of sudden, unpredictable hair loss affecting any scalp area.

Essential Blood Tests for Hair Loss Diagnosis
Comprehensive blood tests form the cornerstone of accurate hair loss diagnosis, revealing underlying conditions that standard examinations often miss. A complete thyroid panel including TSH, free T3, and free T4 identifies thyroid disease affecting up to 20% of hair loss patients, with optimal TSH levels between 0.4-2.5 mIU/L proving crucial for hair growth [9]. Beyond basic thyroid screening, reverse T3 and thyroid antibodies detect subclinical dysfunction that manifests primarily through diffuse thinning.
Iron studies require careful interpretation, as ferritin levels below 70 ng/mL correlate with telogen effluvium even when red blood cells appear normal [3]. Complete panels should include serum iron, transferrin saturation, and total iron-binding capacity to distinguish true deficiency from inflammation-related changes. Hormonal imbalance testing encompasses testosterone, DHEA-S, and sex hormone-binding globulin, whilst diabetes screening through HbA1c identifies metabolic contributors.
Insurance typically covers basic panels when medically indicated, though comprehensive testing averaging £300-500 privately often proves cost-effective by preventing years of ineffective treatments. Test results guide targeted interventions: iron supplementation for deficiency, levothyroxine for hypothyroidism, or metformin for insulin resistance, transforming treatment outcomes when blood work directs therapy.
The Hair Pull Test and Scalp Examination Methods
During a dermatology office visit, the hair pull test remains the cornerstone of the physical exam, where your specialist gently grasps 40-60 hairs between thumb and fingers, applying steady traction to assess shedding patterns. More than six hairs released indicates active loss requiring further investigation, whilst the card test involves placing white card against the scalp to examine hair density and follicular units more clearly under direct lighting.
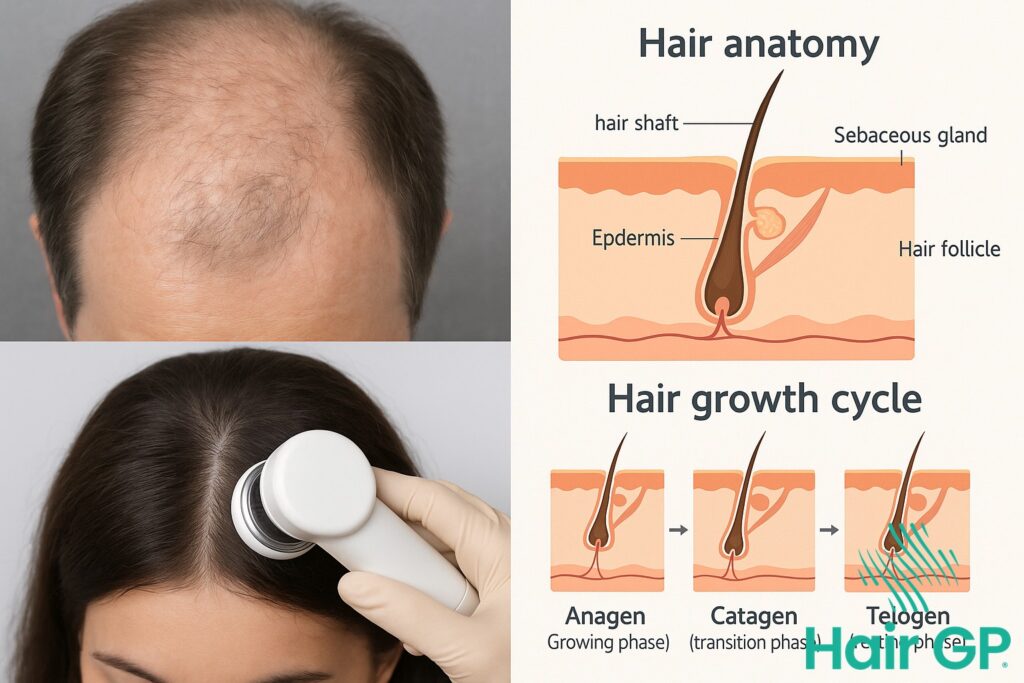
Advanced techniques may include dermoscopy, where a handheld microscope reveals miniaturisation patterns invisible to the naked eye, helping differentiate between scarring and non-scarring alopecias. When diagnosis remains uncertain, a scalp biopsy becomes necessary—typically a 4mm punch biopsy taken under local anaesthetic to examine follicle structure microscopically. Preparing for your appointment by avoiding hair washing for 24 hours and documenting shedding patterns helps your specialist conduct more accurate assessments, as clean hair may yield false-negative pull test results that delay proper diagnosis.

Latest Clinical Trials and Emerging Hair Growth Treatments
Current clinical trials demonstrate promising advances in hair growth therapies beyond traditional treatments. JAK inhibitors, particularly baricitinib, have shown remarkable efficacy in severe alopecia areata, achieving significant regrowth in previously unresponsive cases[10]. These studies revealed that 36% of participants achieved near-complete hair restoration after 36 weeks. Research into platelet-rich plasma combined with microneedling has demonstrated enhanced follicular regeneration, with evidence supporting synergistic effects when used alongside approved medications[11].
Alternative therapies including low-level laser therapy show increasing scientific validation, though further research clarifies optimal parameters. Exosome-based treatments represent emerging frontiers, with preliminary trials indicating follicle-stimulating properties. FDA approval processes typically require multi-phase trials spanning 3-7 years, affecting accessibility. Trial enrollment necessitates precise diagnostic confirmation through trichoscopy, ensuring appropriate patient selection. Realistic expectations remain crucial, as new hair growth patterns vary significantly between individuals and conditions.
Preventing Treatment Failure Through Proper Hair Care
Supporting your hair loss treatment requires mindful hair care practices that prevent additional damage whilst treatments take effect. Choose gentle shampoo and conditioners. Washing hair 2-3x a week is optimal for most and won’t accelerate hair loss when using appropriate products—in fact, clean follicles respond better to treatments.
Avoid tight hairstyles and heavy hair extensions that create traction damage and hair breakage. When you brush, start from the scalp working down with a wide-tooth comb, never forcing through tangles. Heat styling products should include protective sprays, keeping temperatures below 150°C. Most importantly, consistency matters—skipping treatments or returning to damaging practices undermines progress, potentially wasting months of careful restoration efforts.
Conclusion
Understanding the true cause of your hair loss proves essential for selecting the most effective treatment approach. Throughout this guide, we’ve explored various diagnostic tools—from trichoscopy and pull tests to blood work and scalp biopsies—each offering unique insights into different hair loss conditions. Whilst some patterns may seem obvious, an accurate diagnosis requires professional expertise to distinguish between similar-presenting conditions and identify underlying factors that could prevent hair loss progression.
Self-diagnosis often leads to inappropriate treatments that waste valuable time whilst hair loss advances. Hair restoration specialists possess the knowledge and tools to evaluate your specific situation comprehensively, considering medical history, lifestyle factors, and microscopic follicle analysis. Their expertise ensures you receive targeted treatment options tailored to your condition’s root cause, whether addressing nutritional deficiencies, hormonal imbalances, or autoimmune responses.
Rather than experimenting with over-the-counter solutions that may prove ineffective or potentially harmful, schedule a consultation with a qualified hair loss specialist. Professional evaluation represents your first step towards successful hair restoration, providing the accurate diagnosis necessary for truly effective treatment outcomes.
Frequently Asked Questions
Yes, many people regrow hair once the underlying cause is properly diagnosed and treated. Hair regrowth depends on the type of hair loss – conditions like telogen effluvium often fully reverse, while androgenetic alopecia may stabilize with proper treatment. Early diagnosis before permanent follicle damage is crucial for the best outcomes.
Don’t wait more than 3 months if you notice increased hair shedding, thinning hair, or bald patches. Early intervention prevents permanent hair loss and scarring alopecia. See a specialist immediately for sudden patchy hair loss, scalp pain, or inflammation.
Scarring alopecia like lichen planopilaris and frontal fibrosing alopecia permanently destroys hair follicles, causing irreversible hair loss. Non-scarring types preserve follicles, allowing potential regrowth with treatment. Only proper diagnosis through scalp biopsy can differentiate these conditions.
References
- Rossi A, Anzalone A, Fortuna MC, et al. Multi-therapies in androgenetic alopecia: review and clinical experiences. Dermatol Ther. 2016;29(6):424-432.
- Kanti V, Messenger A, Dobos G, et al. Evidence-based (S3) guideline for the treatment of androgenetic alopecia in women and in men – short version. J Eur Acad Dermatol Venereol. 2018;32(1):11-22.
- Trost LB, Bergfeld WF, Calogeras E. The diagnosis and treatment of iron deficiency and its potential relationship to hair loss. J Am Acad Dermatol. 2006;54(5):824-844.
- Gerkowicz A, Chyl-Surdacka K, Krasowska D, Chodorowska G. The Role of Vitamin D in Non-Scarring Alopecia. Int J Mol Sci. 2017;18(12):2653.
- Kanti V, Messenger A, Dobos G, et al. Evidence-based (S3) guideline for the treatment of androgenetic alopecia in women and in men. J Eur Acad Dermatol Venereol. 2018;32(1):11-22.
- York K, Meah N, Bhoyrul B, Sinclair R. A review of the treatment of male pattern hair loss. Expert Opin Pharmacother. 2020;21(5):603-612.
- Zhou C, Li X, Wang C, Zhang J. Alopecia Areata: an Update on Etiopathogenesis, Diagnosis, and Management. Clin Rev Allergy Immunol. 2021;61(3):403-423.
- Strazzulla LC, Wang EHC, Avila L, et al. Alopecia areata: An appraisal of new treatment approaches and overview of current therapies. J Am Acad Dermatol. 2018;78(1):15-24.
- van Beek N, Bodó E, Kromminga A, et al. Thyroid Hormones Directly Alter Human Hair Follicle Functions. J Clin Endocrinol Metab. 2008;93(11):4381-4388.
- King B, Ko J, Forman S, et al. Efficacy and safety of the oral Janus kinase inhibitor baricitinib in the treatment of adults with alopecia areata: Phase 3 results from two randomized controlled trials (BRAVE-AA1 and BRAVE-AA2). J Am Acad Dermatol. 2022;87(2):306-313.
- Gentile P, Garcovich S. Systematic Review: Adipose-Derived Mesenchymal Stem Cells, Platelet-Rich Plasma and Biomaterials as New Regenerative Strategies in Chronic Skin Wounds and Soft Tissue Defects. Int J Mol Sci. 2021;22(15):7851.

")
